Partogram in Obstetrics Complete Guide for Monitoring Labour Progress
Below is a **single-place, exam-ready, clinically complete, SEO-friendly reference** on **Partogram**, written in a **clear H1–H4 structure** suitable for medical students, nurses, midwives, and clinicians.
---
# **Partogram in Obstetrics: Complete Guide for Monitoring Labour Progress**
## **Introduction to Partogram**
A **partogram (partograph)** is a **graphical tool** used to **monitor the progress of labour**, assess **maternal and fetal well-being**, and guide **timely clinical interventions**. It is a **WHO-recommended, low-cost, high-impact tool** for preventing **prolonged and obstructed labour**, thereby reducing **maternal and perinatal morbidity and mortality**.
---
## **Definition of Partogram**
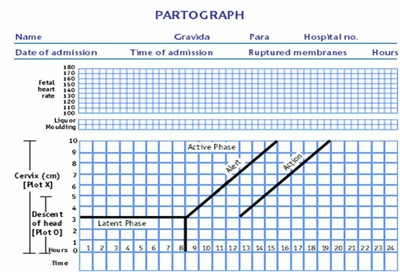
A **partogram** is a **chart that plots cervical dilatation against time**, along with **uterine contractions, fetal condition, and maternal parameters**, to provide a **continuous visual record of labour**.
---
## **Objectives of Using a Partogram**
* Detect **abnormal labour progress early**
* Identify **prolonged labour**
* Prevent **obstructed labour**
* Reduce **maternal complications** (PPH, sepsis, uterine rupture)
* Reduce **fetal complications** (birth asphyxia, stillbirth)
* Assist in **decision-making and referral**
---
## **Types of Partogram**
### **1. WHO Modified Partogram**
* **Active phase starts at 4 cm cervical dilatation**
* **Latent phase excluded**
* Most commonly used in clinical practice
### **2. WHO Composite Partogram (Older)**
* Includes **latent and active phase**
* Latent phase up to **8 hours**
* Less commonly used now
### **3. Simplified Partogram**
* Focuses on **key parameters only**
* Used in **low-resource settings**
---
## **Components of a Partogram**
### **A. Fetal Condition**
Monitored to assess fetal well-being.
#### **1. Fetal Heart Rate (FHR)**
* Recorded **every 30 minutes**
* Normal: **110–160 beats/min**
* Abnormal:
* <110 → Bradycardia
* > 160 → Tachycardia
#### **2. Amniotic Fluid**
* **I** – Intact membranes
* **C** – Clear liquor
* **M** – Meconium-stained
* **B** – Blood-stained
#### **3. Moulding of Fetal Skull**
* 0 → Sutures separated
* * → Sutures touching
* ++ → Sutures overlapping (reducible)
* +++ → Sutures overlapping (irreducible) → **danger sign**
---
### **B. Progress of Labour**
#### **1. Cervical Dilatation**
* Plotted with **X**
* Expected rate in active phase: **≥1 cm/hour**
* Starts at **4 cm**
#### **2. Descent of Head**
* Plotted with **O**
* Measured in **fifths palpable abdominally**
* Or by **station (–5 to +5)**
---
### **C. Uterine Contractions**
Recorded **every 30 minutes**:
| Number / 10 min | Interpretation |
| --------------- | ---------------- |
| <2 | Inadequate |
| 3–4 | Adequate |
| ≥5 | Hyperstimulation |
**Duration**:
* <20 sec – Mild
* 20–40 sec – Moderate
* > 40 sec – Strong
---
### **D. Alert Line and Action Line**
#### **Alert Line**
* Drawn from **4 cm to full dilatation at 1 cm/hour**
* Labour to the **left** → Normal
* Crossing → **Slow progress**
#### **Action Line**
* Drawn **4 hours to the right of alert line**
* Crossing → **Immediate intervention required**
---
### **E. Maternal Condition**
#### **1. Pulse**
* Every **30 minutes**
#### **2. Blood Pressure**
* Every **4 hours**
* More frequent if abnormal
#### **3. Temperature**
* Every **2 hours**
#### **4. Urine Examination**
* Volume
* Protein
* Ketones
---
## **Interpretation of Partogram**
### **Normal Labour**
* Cervical dilatation remains **left of alert line**
* Adequate contractions
* Normal fetal heart rate
### **Prolonged Labour**
* Cervical dilatation crosses **alert line**
* Requires:
* Re-assessment
* Amniotomy
* Oxytocin augmentation
* Referral if needed
### **Obstructed Labour**
* Cervical dilatation reaches **action line**
* Features:
* No descent of head
* Severe moulding (+++)
* Maternal exhaustion
* Management:
* Operative delivery (CS / instrumental)
---
## **Indications for Using a Partogram**
* All women in **active labour**
* Especially useful in:
* Primigravida
* Induced labour
* Previous prolonged labour
* Referral cases
---
## **Contraindications / Limitations**
* Not used in **latent phase (<4 cm)**
* Less effective without **trained staff**
* Requires **regular monitoring**
---
## **Advantages of Partogram**
* Simple and cost-effective
* Visual and easy to interpret
* Reduces:
* Prolonged labour
* Obstructed labour
* Unnecessary interventions
* Improves maternal and neonatal outcomes
---
## **Disadvantages**
* Incorrect plotting may mislead decisions
* Requires training and adherence
* Limited use without timely action
---
## **Role of Partogram in Modern Obstetrics**
* Key tool in **Safe Motherhood Initiative**
* Recommended by **WHO, FIGO**
* Essential in **institutional deliveries**
* Supports **evidence-based labour management**
---
## **Exam-Oriented Clinical Pearls**
* **Alert line crossing** → Observe and evaluate
* **Action line crossing** → Act immediately
* **Moulding +++** → Suggests CPD
* **Meconium liquor** → Fetal distress
* **Rate <1 cm/hr** → Prolonged labour
---
## **Conclusion**
The **partogram is a cornerstone of intrapartum care**, enabling **early detection of abnormal labour**, guiding **timely interventions**, and significantly improving **maternal and neonatal outcomes**. Proper understanding and correct use of the partogram are essential skills for all healthcare providers involved in childbirth.
---
If you want next:
* **SEO title, meta description, and keywords**
* **Image-based explanation**
* **25 hard case-based MCQs**
* **HTML CSS JS interactive partogram simulator**
Just tell me 👍
Partogram Case Based MCQs
Exam Mode • 20 Hard Questions • Obstetrics